|
|
|
|
|
|
|
GLAUCOMA
AD ANGOLO APERTO E MORTALITÀ CARDIOVASCOLARE
[OPEN-ANGLE GLAUCOMA AND MORTALITY: THE BARBADOS EYE STUDIES.
Arch Ophthalmol 2008; 126:365-370]
ABSTRACT
OBJECTIVE To evaluate the relationship between open-angle
glaucoma (OAG) and mortality in a black population at 9-years' follow-up.
DESIGN Population-based cohort study of 4092 black participants
(aged 40-84 years at baseline) in the Barbados Eye Studies. Open-angle
glaucoma was defined by visual field defects and optic disc damage,
based on standardized examinations and photograph gradings. Ocular
hypertension was defined by an intraocular pressure greater than
21 mm Hg or treatment, without OAG damage. Mortality was ascertained
from death certificates. Cox proportional hazards regression analyses
determined associations with mortality.
RESULTS After 9 years, 764 (19%) participants were deceased.
Mortality was unrelated to overall OAG at baseline (n = 300) after
adjustment for confounders. However, cardiovascular mortality tended
to increase in persons with previously diagnosed/treated OAG (n
= 141; relative risk [RR], 1.38, P = .07) and was significantly
higher with treatment involving timolol maleate (RR, 1.91, P = .04).
Cardiovascular deaths also tended to increase in persons with ocular
hypertension at baseline (n = 498; RR, 1.28, P = .06).
CONCLUSIONS In this black population, cardiovascular mortality
tended to increase in persons with previously diagnosed/treated
OAG and ocular hypertension. The excess mortality associated with
timolol maleate treatment of OAG, also found in a white population,
warrants further investigation.
|
|
|
|
|
|
MODIFICAZIONI
DEI FATTORI DI RISCHIO CARDIOVASCOLARE E INCIDENZA DI INFARTO NEL
REGNO UNITO
[HOW MUCH OF THE RECENT DECLINE IN THE INCIDENCE OF MYOCARDIAL INFARCTION
IN BRITISH MEN CAN BE EXPLAINED BY CHANGES IN CARDIOVASCULAR RISK
FACTORS? EVIDENCE FROM A PROSPECTIVE POPULATION-BASED STUDY. Circulation
2008; 117:598-604]
ABSTRACT
BACKGROUND The incidence of myocardial infarction (MI) in
Britain has fallen markedly in recent years. Few studies have investigated
the extent to which this decline can be explained by concurrent
changes in major cardiovascular risk factors.
METHODS AND RESULTS The British Regional Heart Study examined
changes in cardiovascular risk factors and MI incidence over 25
years from 1978 in a cohort of 7735 men. During this time, the age-adjusted
hazard of MI decreased by 3.8% (95% confidence interval 2.6% to
5.0%) per annum, which corresponds to a 62% decline over the 25
years. At the same time, after adjustment for age, cigarette smoking
prevalence, mean systolic blood pressure, and mean non-high-density
lipoprotein (HDL) cholesterol decreased, whereas mean HDL cholesterol,
mean body mass index, and physical activity levels rose. No significant
change occurred in alcohol consumption. The fall in cigarette smoking
explained the greatest part of the decline in MI incidence (23%),
followed by changes in blood pressure (13%), HDL cholesterol (12%),
and non-HDL cholesterol (10%). In combination, 46% (approximate
95% confidence interval 23% to 164%) of the decline in MI could
be explained by these risk factor changes. Physical activity and
alcohol consumption had little influence, whereas the increase in
body mass index would have produced a rise in MI risk.
CONCLUSIONS Modest favorable changes in the major cardiovascular
risk factors appear to have contributed to considerable reductions
in MI incidence. This highlights the potential value of population-wide
measures to reduce exposure to these risk factors in the prevention
of coronary heart disease.
CLINICAL PERSPECTIVE
The incidence of myocardial infarction (MI) in Britain has been
falling since the 1970s. We have estimated that after adjustment
for age, the incidence of first MI declined by 62% from 1979 to
2004 in a representative cohort of middle-aged British men. Few
studies have investigated the contribution of changes in major cardiovascular
risk factors to the decline in MI. Combining data on risk factor
changes with data on MI incidence, we found that approximately half
of the decline in MI incidence in this cohort of men could be explained
by favorable population-wide time trends in cigarette smoking, systolic
blood pressure, high-density lipoprotein (HDL) cholesterol, and
non-HDL cholesterol together. A large fall in cigarette smoking
prevalence explained the greatest single part of the decline (23%),
followed by a fall in mean systolic blood pressure (13%), a rise
in HDL cholesterol (12%), and a fall in non-HDL cholesterol (10%);
however, these contributions may be underestimated owing to imprecision.
A marked increase in mean body mass index is likely to have limited
the extent of the decline. The results indicate that population-wide
changes in risk factors have considerable potential for reducing
MI incidence in the United Kingdom and in other locations. In the
United Kingdom, although the future impact of smoking changes may
be limited by the already low smoking prevalence, the potential
benefits of further reductions in population systolic blood pressure
and blood lipid levels, by a combination of dietary and drug management,
are still considerable.
|
|
|
|
|
|
VARIAZIONI
DELLA DISTRIBUZIONE DELL'IMC E DELLA CIRCONFERENZA VITA IN ADULTI
INGLESI DAL 1993/94 AL 2002/03
[CHANGES IN THE DISTRIBUTIONS OF BODY MASS INDEX AND WAIST CIRCUMFERENCE
IN ENGLISH ADULTS, 1993/1994 TO 2002/2003. Int J Obes 2008; 32:527-32]
ABSTRACT
BACKGROUND Obesity rates have increased markedly in recent
years. This study investigated whether increases in adiposity over
the past 10 years in England reflect across-the-board gains in adiposity
or differential effects in subgroups.
METHODS The data were from the Health Surveys for England,
which include home-based measurements of height, weight and waist
circumference in population-representative samples. Mean-difference
(m-d) curves were calculated to examine increases in BMI and central
adiposity at selected percentile points across the distribution
between 1993/4 and 2002/3. The sample comprised 20 246 participants
in 1993/1994 and 11 708 in 2002/2003. Patterning of population adiposity
was examined in relation to gender, age and socioeconomic status
(SES).
RESULTS Both BMI and central adiposity increased markedly
more in the upper part of the distribution, with intermediate increases
in the middle and little change at the lower end of the distribution.
The patterning and magnitude of increases in adiposity were similar
for men and women, and for lower and higher SES groups. Increases
at the top of the distribution were greater for younger adults,
with the 90th percentile of waist circumference increasing by more
than 8 cm in 10 years in young women.
CONCLUSIONS Gains in adiposity have not been equivalent across
the BMI distribution. Thinner people in 2002/3 were almost as thin
as they were 10 years earlier, but fatter people were considerably
fatter. This could represent progressively greater responsiveness
to the 'obesogenic' environment in individuals with higher complements
of susceptibility genes. These population trends have important
implications for future health and services to manage severe obesity.
|
|
|
|
|
|
SINDROME
METABOLICA E RISK SCORE CARDIOVASCOLARE NELLA SINDROME CORONARICA
ACUTA PREMATURA
[THE METABOLIC SYNDROME PREDICTS CARDIOVASCULAR EVENTS IN SUBJECTS
WITH NORMAL FASTING GLUCOSE: RESULTS OF A 15 YEARS FOLLOW-UP IN
A MEDITERRANEAN POPULATION. Atherosclerosis 2008; 197:147-53]
ABSTRACT
BACKGROUND To compare the relative value of metabolic syndrome
(MetS) and cardiovascular risk score estimates in patients with
acute coronary syndromes (ACS) aged <45 years.
PATIENTS AND METHODS Two hundred consecutive patients (183
men, mean age 40.8 +/- 3.5 years) presented with a first-ever ACS,
and 200 age-and sex-matched controls were evaluated. Metabolic syndrome
diagnostic criteria, European Risk SCORE estimation function, and
the Framingham Risk Score (FRS) were assessed in all participants.
RESULTS The prevalence of the MetS was significantly higher
in the patients' group compared with the control group (51.5% vs
26.0%, P < .001). No subjects with a SCORE >1.0% were identified.
The mean 10-year FRS for patients and controls was 13.03% +/- 7.96%
and 10.02 +/- 8.10%, respectively (P < .001), whereas only 22.5%
of ACS patients had a 10-year risk >20.0% compared with 14.5%
of controls (P = .04). After controlling for potential confounders,
MetS was associated with 1.93 (95% CI 1.13-3.28, P = .01) higher
odds of having an ACS. Moreover, the odds had a positive association
with the increasing cumulative number of MetS components. Crude
and adjusted ORs for the FRS were 1.05 (95% CI 1.029-1.08, P = .001)
and 0.98 (95% CI 0.92-1.05, P = NS), respectively.
CONCLUSION Metabolic syndrome is highly associated with ACS
in subjects <45 years of age and seems to be more valuable than
established cardiovascular risk calculators.
|
|
|
|
|
|
SINDROME
METABOLICA ED EVENTI CV IN SOGGETTI CON GLICEMIA A DIGIUNO NELLA
NORMA
[THE RELATIVE VALUE OF METABOLIC SYNDROME AND CARDIOVASCULAR RISK
SCORE ESTIMATES IN PREMATURE ACUTE CORONARY SYNDROMES. Am Heart
J 2008; 155:534-40]
ABSTRACT
AIM The aim of this study was to evaluate the cardiovascular
(CV) risk due to the metabolic syndrome in a 15-year prospective
study of a Sicilian population. In the Mediterranean area obesity
is highly prevalent, but epidemiological data on the metabolic syndrome
are limited.
METHODS AND RESULTS Among the 1351 subjects enrolled in the
"Ventimiglia di Sicilia" epidemiological project, we selected
687 subjects between 35 and 75 years of age; baseline parameters
were assessed and subjects have been followed for 15 years recording
CV events, total and cardiovascular mortality. The metabolic syndrome
was defined according to both the Adult Treatment Panel III and
the International Diabetes Federation criteria. Metabolic syndrome
(ATPIII criteria) was significantly (p < 0.00001) more prevalent
in women (31.5%) than in men (12.4%). The metabolic syndrome increased
the risk of CV events with a hazard ratio of 1.9 (confidence interval
CI; 1.46-2.46). Using a Cox proportional hazards estimation model,
the survival curve of subjects with metabolic syndrome and normal
fasting glucose did not significantly differ from the curve of subjects
with metabolic syndrome and impaired fasting glucose (IFG).
CONCLUSIONS In a 15-year follow-up the metabolic syndrome
is predictive of CV events regardless of the presence of IFG or
diabetes mellitus.
|
|
|
|
|
|
HDL,
APO A-I E RISCHIO CORONARICO
[HIGH-DENSITY LIPOPROTEIN CHOLESTEROL, HIGH-DENSITY LIPOPROTEIN
PARTICLE SIZE, AND APOLIPOPROTEIN A-I: SIGNIFICANCE FOR CARDIOVASCULAR
RISK IN THE IDEAL AND EPIC-NORFOLK STUDIES. J Am Coll Cardiol 2008;
51:634-42]
ABSTRACT
OBJECTIVES This study was designed to assess the relationship
of high-density-lipoprotein cholesterol (HDL-C), HDL particle size,
and apolipoprotein A-I (apoA-I) with the occurrence of coronary
artery disease (CAD), with a focus on the effect of very high values
of these parameters.
BACKGROUND High plasma levels of HDL-C and apoA-I are inversely
related to the risk of CAD. However, recent data suggest that this
relationship does not hold true for very high HDL-C levels, particularly
when a preponderance of large HDL particles is observed.
METHODS We conducted a post-hoc analysis of 2 prospective
studies: the IDEAL (Incremental Decrease in End Points through Aggressive
Lipid Lowering; n = 8,888) trial comparing the efficacy of high-dose
to usual-dose statin treatment for the secondary prevention of cardiovascular
events, and the EPIC (European Prospective Investigation into Cancer
and Nutrition)-Norfolk case-control study, including apparently
healthy individuals who did (cases, n = 858) or did not (control
patients, n = 1,491) develop CAD during follow-up. In IDEAL, only
HDL-C and apoA-I were available; in EPIC-Norfolk, nuclear magnetic
resonance spectroscopy-determined HDL particle sizes were also available.
RESULTS In the IDEAL study, higher HDL-C proved a significant
major cardiac event risk factor following adjustment for age, gender,
smoking, apoA-I, and apoB. A similar association was observed for
HDL particle size in EPIC-Norfolk. Increased risk estimates were
particularly present in the high ends of the distributions. In contrast,
apoA-I remained negatively associated across the major part of its
distribution in both studies.
CONCLUSIONS When apoA-I and apoB are kept constant, HDL-C
and HDL particle size may confer risk at very high values. This
does not hold true for very high levels of apoA-I at fixed levels
of HDL-C and apoB. These findings may have important consequences
for assessment and treatment of CAD risk.
|
|
|
|
|
|
FATTORI
DI RISCHIO PER LO SVILUPPO DI SINDROME CORONARICA ACUTA
[SEX DIFFERENCES IN CARDIOVASCULAR RISK FACTORS AND THE IMPACT
OF SEX ON THE OCCURRENCE OF AN ACUTE CORONARY EVENT. A CASE-CONTROL
STUDY. Eur J Cardiovasc Nurs 2008; 7:S12-S13]
ABSTRACT
INTRODUCTION The role of sex on the development of atherosclerosis
has long been recognized. In this work we aimed to evaluate the
extent to which cardiovascular risk factors can explain the sex
difference in coronary heart disease (CHD) risk.
METHODS During 2000-01, we randomly selected from all Greek
regions 848 hospitalised patients with a first event of an acute
coronary syndrome and 1078 paired, by sex, age, and region controls,
without any suspicious for CHD. All participants were evaluated
through a rather detailed questionnaire in which demographic,
athropometric, life-style habits; social, psychometric, nutritional
and clinical factors were recorded.
RESULTS Women patients were significantly older than men
(65.3 ± 8 vs. 59.7 ± 10 years old, p < 0.01).
The frequency ratio of males÷females patients was 4÷1.
The effect of the family history of premature CHD and hypercholesterolemia,
on the risk of developing acute coronary syndromes, seems to be
related more consistent in males, while the presence of hypertension
affects more significantly females. The higher education level
as well as the adoption of Mediterranean diet seems to be more
protective in females, while, depression is associated with higher
risk of developing ACS in women.
CONCLUSION Lifestyle characteristics as well as several
clinical symptoms and laboratory measurements seem to play significant
role in the distinction of the risk factors profile between sexes.
However, much remains to be learned about the mechanisms that
relate CHD risk and sex.
[FISH CONSUMPTION AND THE RISK OF DEVELOPING ACUTE CORONARY
SYNDROMES: A CASE-CONTROL STUDY. Eur J Cardiovasc Nurs 2008; 7:S11-S12]
ABSTRACT
OBJECTIVE Diet has been recognized to have an important
role on the development, as well as, the progression of atherosclerosis
The aim of this work was to investigate the association between
fish consumption and the development of non-fatal acute coronary
syndromes, in a Mediterranean population.
METHODS During 2000-01, we randomly and stratified selected,
from all Greek regions, 848 hospitalised patients (695 males,
58 ± 10 years old and 153 females, 65 ± 9 years
old) who had a first event of acute coronary syndromes (ACS) and
1078 paired, by region-sex-age, controls without any clinical
symptoms or signs of coronary heart disease.
RESULTS On multivariate logistic regression analysis, and
after controlling for several potential confounders, we found
that fish consumption less than 150 g/wk was associated with 38%
lower odds of developing ACS as compared to no consumption (odds
ratio = 0.62, P -value < 0.05). In contrast, moderate (150-300
g/wk) and high (> 300 g/wk) fish consumption was not associated
with the developing of the disease (odds ratios = 1.10 and 1.01,
respectively, P -value > 0.1). The benefits from low fish consumption
were also significant even amongst current smokers and diabetics.
CONCLUSION Moderate fish consumption was independently
associated with a significant reduction in the odds of developing
ACS. The strength and consistency of this finding has implications
for public health and should be explored further.
[THE IMPACT OF PHYSICAL ACTIVITY ON THE RISK OF DEVELOPMENT
AN ACUTE CORONARY SYNDROME, IN HYPERTENSIVE SUBJECTS. Eur J Cardiovasc
Nurs 2008; 7:S13]
ABSTRACT
INTRODUCTION The level of blood pressure is known to determinate
the cardiovascular risk. In this work we aimed to evaluate the
effect of physical exercise on the coronary risk, in different
groups of hypertensives.
METHODS During 2000-01, we randomly selected 848 hospitalised
patients (695 males, 58 ± 10-153 females, 65 ± 9
years old) with a first event of coronary heart disease (CHD)
and 1078 paired, by sex-age, hospitalised controls without CHD.
Physically active was defined as those who reported non-occupational
physical activity > 1/week. The rest were considered physically
inactive.
RESULTS 418 (49%) of the patients and 303 (28%) of the
controls were hypertensive. Of them 21 (5%) patients-36 (12%)
controls were unaware of their condition, 94 (22%)-34 (11%) were
untreated, 148 (35%)-111 (36%) were uncontrolled and 155 (38%)-122
(41%) were controlled (P - < 0.01). Two hundred eighty-eight
(34%) of the patients and 453 (42%) controls were assigned to
light (13% vs. 17%, respectively, P < 0.01), moderate (7% vs.
13%, P < 0.01) and vigorous physical activity level (14% vs.
12%, P = 0.078). The adoption of moderate physical activity reduced
by 21% the coronary risk in controlled hypertensive subjects (OR
= 0.79, P < 0.01), by 13% (OR = 0.87, P < 0.05) in uncontrolled
and by 7% (OR = 0.93, P < 0.05) in unaware of their condition,
after adjusting for age, sex, educational and financial level
and the conventional cardiovascular risk factors.
CONCLUSION The adoption of physical activity is associated
with reduction of the coronary risk in hypertensives. Non-habitual
exercise seems to prevent approximately, one fourth of the acute
coronary events due to hypertension, in controlled hypertensive
subjects.
[THE ROLE OF PHYSICAL ACTIVITY ON THE DEVELOPMENT OF ACUTE
CORONARY SYNDROMES IN DIABETIC PATIENTS. A CASE-CONTROL STUDY.
Eur J Cardiovasc Nurs 2008; 7:S12]
ABSTRACT
BACKGROUND Epidemiological data suggest that the prevalence
of type-2 diabetes is increasing dramatically, especially, during
the past years. This increase is primarily being driven by environmental
factors, like dietary and exercise habits. In this study we investigated
the effect of physical activity on coronary risk, in diabetic
patients, an issue that has not been adequately studied so far.
METHODS We studied demographic, lifestyle, dietary and
clinical information in 216 hospitalized diabetic patients (171
men, 63 ± 9 years old and 45 women, 67 ± 5 years
old) with a first event of an acute coronary syndrome (ACS) and
196 frequency matched (by age and sex) diabetic controls (154
men, 64 ± 11 years old and 42 women, 66 ± 6 years
old) without any clinical evidence of CHD (from the CARDIO2000
II study). Diabetes mellitus was defined according to the established
ADA criteria. Physically active were considered those who reported
non-occupational physical activity > 1 time/week (at least
30 min/time). The rest were considered physically inactive. Physical
activity was evaluated according to the Kcal/min expended and
the weekly frequency of exercise.
RESULTS Seventy-eight (36%) of 216 patients and 110 (56%)
of 196 controls were classified as physically active (p < 0.001).
Multivariate conditional logistic regression analysis revealed
that the odds ratio for developing an acute coronary event in
diabetic subjects who reported moderate level of physical activity
was 0.22 (95% CI 0.12-0.47), while the odds ratio in diabetics
who reported high level was 0.33 (95% CI 0.21-0.59), after adjusting
for age, sex, and the conventional cardiovascular risk factors.
CONCLUSIONS Physical activity (moderate and high level)
seems to be associated with a lower coronary risk in the investigated
group of diabetic subjects. Light physical activity does not seem
to confer any protective effect.
|
|
|
|
|
|
DILATAZIONE
FLUSSO-MEDIATA DELLE ARTERIE BRACHIALI E FATTORI DI RISCHIO CARDIACI
IN DONNE IN MENOPAUSA
[PROGNOSTIC ROLE OF FLOW-MEDIATED DILATION AND CARDIAC RISK FACTORS
IN POST-MENOPAUSAL WOMEN. J Am Coll Cardiol 2008; 51:997-1002]
ABSTRACT
OBJECTIVES The aim of this study was to examine the association
between brachial artery flow-mediated dilation (FMD) and cardiovascular
events in a cohort of initially asymptomatic post-menopausal women,
with adjustment for the presence of the major cardiovascular risk
factors.
BACKGROUND Conventional major cardiovascular risk factors
(cigarette smoking, hypercholesterolemia, hypertension, and diabetes)
fail to explain nearly 50% of cardiovascular events. Defining the
magnitude of future risk for the development of clinical events
is a major focus of effective primary prevention. Evaluation of
endothelial function, utilizing the noninvasive measurement of the
brachial artery FMD, may serve as a screening tool to individualize
high-risk patients.
METHODS We conducted a prospective study on 2,264 post-menopausal
women, age 54 +/- 6 years. The length of the follow-up was 45 +/-
13 months (range 6 to 65 months). RESULTS: During observation, 90
major events were recorded. Risk-adjusted relative risk values resulted
1.0, 1.33 (95% confidence interval [CI] 1.09 to 4.09), and 4.42
(95% CI 2.97 to 8.01) for women in the higher, intermediate, and
lower tertile of FMD, respectively (p < 0.0001 for trend). The
event rate for women in the lower tertile (FMD <or=4.5%) was
greater than the combined event rate noted in the other 2 tertiles
(women in the lower tertile accounted for 51 events [56.6% of total
events]). When added to age and other conventional cardiovascular
risk factors (smoking habits, presence of hypercholesterolemia,
history of diabetes, hypertension), FMD contributed significantly
to the model predicting cardiovascular events (likelihood ratio
chi-square change: 10.22; p < 0.0001).
CONCLUSIONS In post-menopausal women, the knowledge of FMD
provided incremental prognostic information regarding the risk of
developing cardiovascular events.
|
|
|
|
|
|
MASSA
VENTRICOLARE SINISTRA E INSUFFICIENZA CARDIACA
[LEFT VENTRICULAR MASS PREDICTS HEART FAILURE NOT RELATED TO PREVIOUS
MYOCARDIAL INFARCTION: THE CARDIOVASCULAR HEALTH STUDY . Eur Heart
J 2008; 29:741-747]
ABSTRACT
AIMS The relationship of left ventricular hypertrophy (LVH)
to incident heart failure (HF) not attributable to myocardial infarction
(MI) has not been defined. We assessed whether LVH is an independent
predictor of MI-independent HF.
METHODS AND RESULTS LVH was assessed by echocardiographic
LV mass index (in g/m2.7) and excess of LV mass (eLVM, in % of the
observed value) relative to the amount predicted by sex, stroke
work, and height, using a prognostically validated equation in 2078
participants of Cardiovascular Health Study without prevalent MI
and normal systolic function. Increasing eLVM was associated with
progressively increasing left atrial dimension and concentric geometry,
decreasing systolic (P < 0.0001), and diastolic function (P <
0.04). After adjustment for age, sex, obesity, diabetes, hypertension,
and antihypertensive therapy, and accounting for by incident MI,
hazard of HF increased by 1% for each 1% increase in eLVM and by
3% for each g/m2.7 increase in LV mass index (both P < 0.0001).
The results were confirmed when also C-reactive protein and measures
of systolic (endocardial shortening) and diastolic function (categories
of E/A ratio) were added to the Cox models.
CONCLUSION In an elderly population, LVH, measured as LV
mass index or eLVM is an independent predictor of incident HF not
related to prevalent or incident MI.
|
|
|
|
|
|
GRASSO
EPICARDICO PERICORONARICO E CALCIFICAZIONE CORONARICA
[PERI-CORONARY EPICARDIAL ADIPOSE TISSUE IS RELATED TO CARDIOVASCULAR
RISK FACTORS AND CORONARY ARTERY CALCIFICATION IN POST-MENOPAUSAL
WOMEN . Eur Heart J 2008; 29:777-783]
ABSTRACT
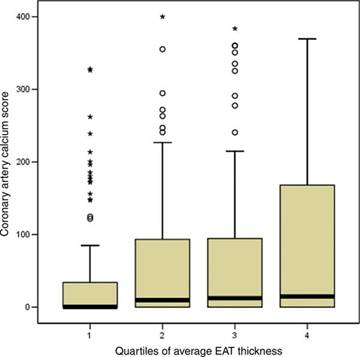
AIMS To determine whether peri-coronary epicardial adipose
tissue (EAT) is associated with vascular risk factors and coronary
atherosclerosis.
METHODS AND RESULTS In this study, 573 healthy post-menopausal
women underwent a cardiac CT scan to assess coronary calcification.
Peri-coronary EAT thickness was measured in the areas of right
coronary artery (RCA), left anterior descending (LAD) artery,
and left circumflex (LCX) coronary artery. Average EAT thickness
was 16.5 ± 4.3 mm (range 5.9-34.6) in the RCA area, 6.4
± 2.2 mm (range 2.0-14.0) in the LAD area, and 10.8 ±
3.0 mm (range 2.8-29.1) in the LCX area. Overall average thickness
was 11.2 ± 2.2 mm (range 5.4-19.1). EAT was positively
related to age (P = 0.002). In age-adjusted linear regression
models, EAT was positively related to weight (P< 0.001), waist
circumference (P< 0.001), waist-to-hip ratio (P< 0.001),
body mass index (P< 0.001), glucose (P< 0.001), triglycerides
(P = 0.001), use of anti-hypertensive drugs (P = 0.007), and systolic
blood pressure (P = 0.034), and inversely to HDL cholesterol (P
= 0.005). In multivariable models, age, weight, waist circumference,
smoking, and glucose were the main determinants of EAT. EAT showed
a graded relation with coronary calcification (P = 0.026).
CONCLUSION EAT is strongly related to vascular risk factors
and coronary calcification. Our findings support the hypothesis
that EAT affects coronary atherosclerosis and possibly coronary
risk.
Coronary
artery calcification scores by peri-coronary epicardial adipose
tissue quartile
[PERICARDIAL
FAT, VISCERAL ABDOMINAL FAT, CARDIOVASCULAR DISEASE RISK FACTORS,
AND VASCULAR CALCIFICATION IN A COMMUNITY-BASED SAMPLE: THE FRAMINGHAM
HEART STUDY. Circulation 2008; 117:605-13]
ABSTRACT
BACKGROUND Pericardial fat may be an important mediator
of metabolic risk. Correlations with cardiovascular disease risk
factors and vascular calcification in a community-based sample
are lacking. We sought to examine associations between pericardial
fat, metabolic risk factors, and vascular calcification.
METHODS AND RESULTS Participants free of cardiovascular
disease from the Framingham Heart Study (n=1155, mean age 63 years,
54.8% women) who were part of a multidetector computed tomography
study underwent quantification of intrathoracic fat, pericardial
fat, visceral abdominal fat (VAT), coronary artery calcification,
and aortic artery calcification. Intrathoracic and pericardial
fat volumes were examined in relation to body mass index, waist
circumference, VAT, metabolic risk factors, coronary artery calcification,
and abdominal aortic calcification. Intrathoracic and pericardial
fat were directly correlated with body mass index (r=0.41 to 0.51,
P<0.001), waist circumference (r=0.43 to 0.53, P<0.001),
and VAT (r=0.62 to 0.76, P<0.001). Both intrathoracic and pericardial
fat were associated with higher triglycerides (P<0.0001), lower
high-density lipoprotein (P<0.0001), hypertension (P<0.0001
to 0.01), impaired fasting glucose (P<0.0001 to 0.001), diabetes
mellitus (P=0.0005 to 0.009), and metabolic syndrome (P<0.0001)
after multivariable adjustment. Associations generally persisted
after additional adjustment for body mass index and waist circumference
but not after adjustment for VAT (all P>0.05). Pericardial
fat, but not intrathoracic fat, was associated with coronary artery
calcification after multivariable and VAT adjustment (odds ratio
1.21, 95% confidence interval 1.005 to 1.46, P=0.04), whereas
intrathoracic fat, but not pericardial fat, was associated with
abdominal aortic calcification (odds ratio 1.32, 95% confidence
interval 1.03 to 1.67, P=0.03).
CONCLUSIONS Pericardial fat is correlated with multiple
measures of adiposity and cardiovascular disease risk factors,
but VAT is a stronger correlate of most metabolic risk factors.
However, intrathoracic and pericardial fat are associated with
vascular calcification, which suggests that these fat depots may
exert local toxic effects on the vasculature.
|
|
|
|
|
|
POLIMORFISMI
E RISCHIO DI EVENTI CARDIOVASCOLARI
[POLYMORPHISMS ASSOCIATED WITH CHOLESTEROL AND RISK OF CARDIOVASCULAR
EVENTS. N Engl J Med 2008 ; 358:1240-9]
ABSTRACT
BACKGROUND Common single-nucleotide polymorphisms (SNPs)
that are associated with blood low-density lipoprotein (LDL) or
high-density lipoprotein (HDL) cholesterol modestly affect lipid
levels. We tested the hypothesis that a combination of such SNPs
contributes to the risk of cardiovascular disease.
METHODS We studied SNPs at nine loci in 5414 subjects from
the cardiovascular cohort of the Malmö Diet and Cancer Study.
We first validated the association between SNPs and either LDL
or HDL cholesterol and subsequently created a genotype score on
the basis of the number of unfavorable alleles. We used Cox proportional-hazards
models to determine the time to the first cardiovascular event
in relation to the genotype score.
RESULTS All nine SNPs showed replication of an association
with levels of either LDL or HDL cholesterol. With increasing
genotype scores, the level of LDL cholesterol increased from 152
mg to 171 mg per deciliter (3.9 to 4.4 mmol per liter), whereas
HDL cholesterol decreased from 60 mg to 51 mg per deciliter (1.6
to 1.3 mmol per liter). During follow-up (median, 10.6 years),
238 subjects had a first cardiovascular event. The genotype score
was associated with incident cardiovascular disease in models
adjusted for covariates including baseline lipid levels (P<0.001).
The use of the genotype score did not improve the clinical risk
prediction, as assessed by the C statistic. However, there was
a significant improvement in risk classification with the use
of models that included the genotype score, as compared with those
that did not include the genotype score.
CONCLUSIONS A genotype score of nine validated SNPs that
are associated with modulation in levels of LDL or HDL cholesterol
was an independent risk factor for incident cardiovascular disease.
The score did not improve risk discrimination but did modestly
improve clinical risk reclassification for individual subjects
beyond standard clinical factors.
|
|
|
|
|
|
DISTURBI
RESPIRATORI NEL SONNO E RISCHIO CARDIOVASCOLARE
[RELATION OF SLEEP-DISORDERED BREATHING TO CAROTID PLAQUE AND INTIMA-MEDIA
THICKNESS. Atherosclerosis 2008; 197:125-131 ]
ABSTRACT
BACKGROUND Sleep-disordered breathing (SDB) is associated
with clinical cardiovascular disease (CVD), but its relation to
subclinical atherosclerosis remains to be determined.
METHODS We analyzed the cross-sectional associations of SDB,
measured by the respiratory disturbance index (RDI), a hypoxemia
index, and an arousal index, with carotid plaque and carotid intima-media
thickness (IMT), measured by ultrasound. The sample included 985
participants in the Sleep Heart Health Study (mean age-62, median
RDI-8.7) with no history of coronary heart disease and stroke, of
whom 396 had evidence of a carotid plaque.
RESULTS As compared with the first quartile of the RDI (0-1.2),
the crude odds ratio for carotid plaque was 1.14, 1.27, and 1.48
for the second (1.3-4.1), third (4.2-10.7), and fourth (>10.7)
quartile, respectively. After adjustment for CVD risk factors, the
corresponding odds ratios were reduced (1.00, 1.04, 1.07, and 1.25).
Similarly, the unadjusted mean carotid IMT increased with RDI, but
adjusted means (mm) were similar (0.84, 0.85, 0.84, 0.85). Spline
regression models did not show monotonicity of the dose-response
functions at the right end of the RDI distribution. Neither the
hypoxemia index nor the arousal index was associated with carotid
plaque or carotid IMT.
CONCLUSION The results of this study suggest that crude,
positive associations between SDB and subclinical atherosclerosis
can be attributed to confounding by CVD risk factors.
[OBSTRUCTIVE SLEEP APNEA IS A RISK FACTOR FOR DEATH IN PATIENTS
WITH STROKE: A 10-YEAR FOLLOW-UP. Arch Intern Med 2008; 168:297-301]
ABSTRACT
BACKGROUND Sleep apnea occurs frequently among patients with
stroke, but it is still unknown whether a diagnosis of sleep apnea
is an independent risk factor for mortality. We aimed to investigate
whether obstructive or central sleep apnea was related to reduced
long-term survival among patients with stroke.
METHODS Of 151 patients admitted for in-hospital stroke rehabilitation
in the catchment area of Umeå from April 1, 1995, to May 1,
1997, 132 underwent overnight sleep apnea recordings at a mean (SD)
of 23 (8) days after the onset of stroke. All patients were followed
up prospectively for a mean (SD) of 10.0 (0.6) years, with death
as the primary outcome; no one was lost to follow-up. Obstructive
sleep apnea was defined when the obstructive apnea-hypopnea index
was 15 or greater, and central sleep apnea was defined when the
central apnea-hypopnea index was 15 or greater. Patients with obstructive
and central apnea-hypopnea indexes of less than 15 served as control
subjects.
RESULTS Of 132 enrolled patients, 116 had died at follow-up.
The risk of death was higher among the 23 patients with obstructive
sleep apnea than controls (adjusted hazard ratio, 1.76; 95% confidence
interval, 1.05-2.95; P = .03), independent of age, sex, body mass
index, smoking, hypertension, diabetes mellitus, atrial fibrillation,
Mini-Mental State Examination score, and Barthel index of activities
of daily living. There was no difference in mortality between the
28 patients with central sleep apnea and controls (adjusted hazard
ratio, 1.07; 95% confidence interval, 0.65-1.76; P = .80).
CONCLUSIONS Patients with stroke and obstructive sleep apnea
have an increased risk of early death. Central sleep apnea was not
related to early death among the present patients.
|
|
|
|
|
|
CONSUMO
MODERATO DI ALCOLICI IN MEZZA ETÀ ED EVENTI CARDIOVASCOLARI
[ADOPTING MODERATE ALCOHOL CONSUMPTION IN MIDDLE AGE: SUBSEQUENT
CARDIOVASCULAR EVENTS. Am J Med 2008; 121:201-236]
ABSTRACT
PURPOSE Moderate alcohol use is part of a healthy lifestyle,
yet current guidelines caution nondrinkers against starting to drink
alcohol in middle age. The purpose of this study was to evaluate
whether adopting moderate alcohol consumption in middle age would
result in subsequent lower cardiovascular risk.
METHODS This study examined a cohort of adults aged 45-64
years participating in the Atherosclerosis Risk in Communities study
over a 10-year period. The primary outcome was fatal or nonfatal
cardiovascular events.
RESULTS Of 7697 participants who had no history of cardiovascular
disease and were nondrinkers at baseline, within a 6-year follow-up
period, 6.0% began moderate alcohol consumption (2 drinks per day
or fewer for men, 1 drink per day or fewer for women) and 0.4% began
heavier drinking. After 4 years of follow-up, new moderate drinkers
had a 38% lower chance of developing cardiovascular disease than
did their persistently nondrinking counterparts. This difference
persisted after adjustment for demographic and cardiovascular risk
factors (odds ratio 0.62, 95% confidence interval, 0.40-0.95). There
was no difference in all-cause mortality between the new drinkers
and persistent nondrinkers (odds ratio 0.71, 95% confidence interval,
0.31-1.64).
CONCLUSION People who newly begin consuming alcohol in middle
age rarely do so beyond recommended amounts. Those who begin drinking
moderately experience a relatively prompt benefit of lower rates
of cardiovascular disease morbidity with no change in mortality
rates after 4 years.
|
|
|
|
| |
DIFFERENZE
DI ETÀ E SESSO NELL'IMPATTO DEL DIABETE E NELLA PREVALENZA
DI PATOLOGIA ISCHEMICA
[AGE AND GENDER DIFFERENCES IN THE IMPACT OF DIABETES ON THE PREVALENCE
OF ISCHEMIC HEART DISEASE: A POPULATION-BASED REGISTER STUDY. Diabetes
Res Clin Pract. 2008 Mar;79(3):497-502]
ABSTRACT
OBJECTIVE To explore age and gender differences in the impact
of diabetes on the prevalence of ischemic heart disease (IHD) in
a defined population.
METHODS Data were obtained from an administrative health
care register covering a population of about 415,000. The study
included all patients aged 45-74 years diagnosed between 1999 and
2003 with IHD (n = 11,311) and diabetes (n = 10,364) by physicians
at all primary health care centres (PHCs) and out- and inpatient
clinics at all hospitals in the county of Östergötland,
Sweden.
RESULTS In the 45-54-year-old age group, diabetes was associated
with an increase in IHD prevalence equivalent to ageing about 20
years in women and 10 years in men. The diabetes/nondiabetes IHD
prevalence rate ratio (IPR) decreased with age in both men and women
(trend p -values <0.001). The IPR was higher among women than
men in each age group, though the female relative excess decreased
from 75% higher in the 45-54-year-old age group to 33% higher in
the 65-74-year-old age group (trend p -value = 0.018).
CONCLUSIONS The relative gender difference in the impact
of diabetes on IHD in younger middle-aged patients remained up to
the age of 65 years, decreasing considerably thereafter.
|
|
|
|
| |
BIOMARKER
DI INFIAMMAZIONE E MORTALITÀ VASCOLARE E NON VASCOLARE
[BIOMARKERS OF INFLAMMATION PREDICT BOTH VASCULAR AND NON-VASCULAR
MORTALITY IN OLDER MEN. Eur Heart J 2008; 29:800-809]
ABSTRACT
AIMS To compare the predictive value of inflammatory biomarkers
and lipids for vascular and non-vascular mortality in older men.
METHODS AND RESULTS The relevance of inflammatory biomarkers
and lipids for vascular and non-vascular mortality was assessed
in a prospective study of 5360 men (mean age 77 years) followed
for 7 years. Vascular mortality was positively associated with log
C-reactive protein (lnCRP), fibrinogen and total/HDL-C (high-density
lipoprotein cholesterol), and inversely associated with albumin
[age adjusted hazard ratio (HR) per 2-SD higher usual level (approximately
the difference between the top and the bottom thirds of the distribution):
2.09 for lnCRP; 1.70 for fibrinogen; 0.50 for albumin and 1.45 for
total/HDL-C]. The associations with the inflammatory markers were
attenuated after adjustment for established risk factors, including
lipids [adjusted HRs: 1.86 (lnCRP); 1.44 (fibrinogen); 0.51 (albumin)],
and further attenuated (and, for fibrinogen, no longer predictive)
after adjustment for each other [fully adjusted HRs: 1.60 (lnCRP);
1.01 (fibrinogen); 0.61 (albumin)]. Higher CRP and lower albumin
levels were also associated with significantly raised non-vascular
mortality independently of other characteristics [fully adjusted
HRs: 1.62 (lnCRP); 0.65 (albumin)].
CONCLUSION In this cohort of older men, higher CRP and lower
albumin levels strongly predicted both vascular and non-vascular
mortality, independently of other characteristics.
|
|
|
|
| |
LIVELLI
PLASMATICI DI SELENIO E MORTALITÀ TOTALE, CARDIOVASCOLARE
E PER TUMORI
[SERUM SELENIUM LEVELS AND ALL-CAUSE, CANCER, AND CARDIOVASCULAR
MORTALITY AMONG US ADULTS. Arch Intern Med 2008; 168:404-10]
ABSTRACT
BACKGROUND Selenium, an essential trace element involved
in defense against oxidative stress, may prevent cancer and cardiovascular
disease. We evaluated the association between selenium levels and
all-cause and cause-specific mortality in a representative sample
of US adults.
METHODS Serum selenium levels were measured in 13,887 adult
participants in the Third National Health and Nutrition Examination
Survey. Study participants were recruited from 1988 to 1994 and
followed up for mortality for up to 12 years.
RESULTS The mean serum selenium level was 125.6 ng/mL. The
multivariate adjusted hazard ratios comparing the highest (>
or = 130.39 ng/mL) with the lowest (< 117.31 ng/mL) serum selenium
level tertile were 0.83 (95% confidence interval [CI], 0.72-0.96)
for all-cause mortality, 0.69 (95% CI, 0.53-0.90) for cancer mortality,
and 0.94 (95% CI, 0.77-1.16) for cardiovascular mortality. However,
based on spline regression models, the association between serum
selenium levels and all-cause and cancer mortality was nonlinear,
with an inverse association at low selenium levels (<130 ng/mL)
and a modest increase in mortality at high selenium levels (>
150 ng/mL). There was no association between serum selenium levels
and cardiovascular mortality.
CONCLUSIONS In a representative sample of the US population,
we found a nonlinear association between serum selenium levels and
all-cause and cancer mortality. Increasing serum selenium levels
were associated with decreased mortality up to 130 ng/mL. Our study,
however, raises the concern that higher serum selenium levels may
be associated with increased mortality.
|
|
|
|
| |
CALCIO,
MAGNESIO, VITAMINA D E VITAMINA K E INCIDENZA DI FRATTURA ALL'ANCA
[ASSOCIATION OF HIP FRACTURE INCIDENCE AND INTAKE OF CALCIUM, MAGNESIUM,
VITAMIN D, AND VITAMIN K. Eur J Epidemiol 2008; 23:219-225]
ABSTRACT
OBJECTIVE To analyze the association between hip fracture
incidence in 12 regional blocks within Japan and dietary intake
of four key nutrients: calcium, magnesium, vitamin D, and vitamin
K.
DESIGN An ecological study. Methods Using data from the 2002
national survey on the incidence of hip fracture and the National
Nutritional Survey of Japan, a standardized incidence ratio of hip
fracture was calculated, and the association between the standardized
incidence ratio and each nutritional intake was assessed for each
region using Pearson's correlation coefficient and partial correlation
analysis.
RESULTS There were significant correlations between the standardized
incidence ratio by region and magnesium, vitamin D, and vitamin
K in both men and women, and calcium in women. The strongest inverse
correlations were found in vitamin K in both men and women (r =
-0.844, P = 0.001, and r = -0.834, P = 0.001, respectively). After
adjusting for calcium, magnesium, and vitamin D, the partial correlation
between the standardized incidence ratio by regional block and vitamin
K was strongest in both men and women (partial correlation coefficient,
pcc = -0.673, P = 0.04; pcc = -0.575, P = 0.106, respectively).
CONCLUSIONS The significant correlation between hip fracture
incidence and vitamin K intake, and also regional variations in
food patterns, suggest that increasing intake of vegetables and
legumes might lead to a decrease in hip fracture incidence in the
future. Further, this study suggests that a review of the dietary
reference value of vitamin K from the perspective of osteoporosis
would be useful.
|
|
|
|
| |
|
|
|
|
| |
|
| |
|
| |
|
|
